

People ask the same question in different words: Do I need therapy, medication, or both? The answer depends on your diagnosis, symptom severity, what you’ve tried before, safety considerations, and what you can realistically maintain.
The APA emphasizes two anchors: use the best available evidence, and choose an option you’re willing to start and stick with in collaboration with a licensed clinician. Take the example of HIPAA-compliant Telehealth. That is the frame for every recommendation here.
What Each Treatment Does (therapy vs medication)
Talk therapy (psychotherapy) works by changing thoughts, behaviors, and relationship patterns that keep symptoms in place. Sessions can be in-person or virtual. Major modalities with the strongest track records include:
- CBT: structured, goal-based skill building; unlearn unhelpful cycles and practice healthier ones.
- DBT: emotion regulation and distress tolerance for people who experience emotions intensely.
- Interpersonal therapy (IPT): short-term work on relationships, roles, and life transitions; strong evidence in major depression.
- Psychodynamic therapy: links past patterns to current symptoms to improve insight and flexibility.
Tele-therapy is useful across anxiety disorders (OCD, phobias, panic, PTSD), mood disorders (depression, bipolar), addictions, eating disorders, personality disorders, and even schizophrenia (for function and coping), as well as for stress, conflict, and life change, diagnosis or not.
Medication management (pharmacotherapy) adjusts brain chemistry to relieve symptoms. The most common classes include:
- Antidepressants (SSRIs/SNRIs, etc.) for depression and many anxiety disorders; typical courses run ≥6 months; potential effects: GI upset, headache, sedation, sexual side effects.
- Benzodiazepines for short-term severe anxiety/panic; controlled substances requiring careful risk screening.
- Mood stabilizers (e.g., lithium, valproate) for bipolar disorder; also for treatment-resistant depression.
- Antipsychotics for schizophrenia and other conditions with psychosis; sometimes used adjunctively in bipolar or depression.
Note: This is not medical advice and is not equivalent to the Doctor’s advice.
Medication may take weeks to show full benefit; dose or agent adjustments are common. (Where appropriate, pharmacogenomic testing can inform choices by showing how a person metabolizes certain medications.)
Your Next Step to Real Relief Starts With CPG
Waiting only makes symptoms worse. Whether you need fast-acting medication, talk therapy, or both, our HIPAA-secure team will guide you toward the relief and long-term stability you deserve.
When Therapy is Recommended First
Evidence favors therapy as first-line for many presentations, especially anxiety disorders, mild–moderate depression, trauma-related conditions, insomnia, and personality-structure problems:
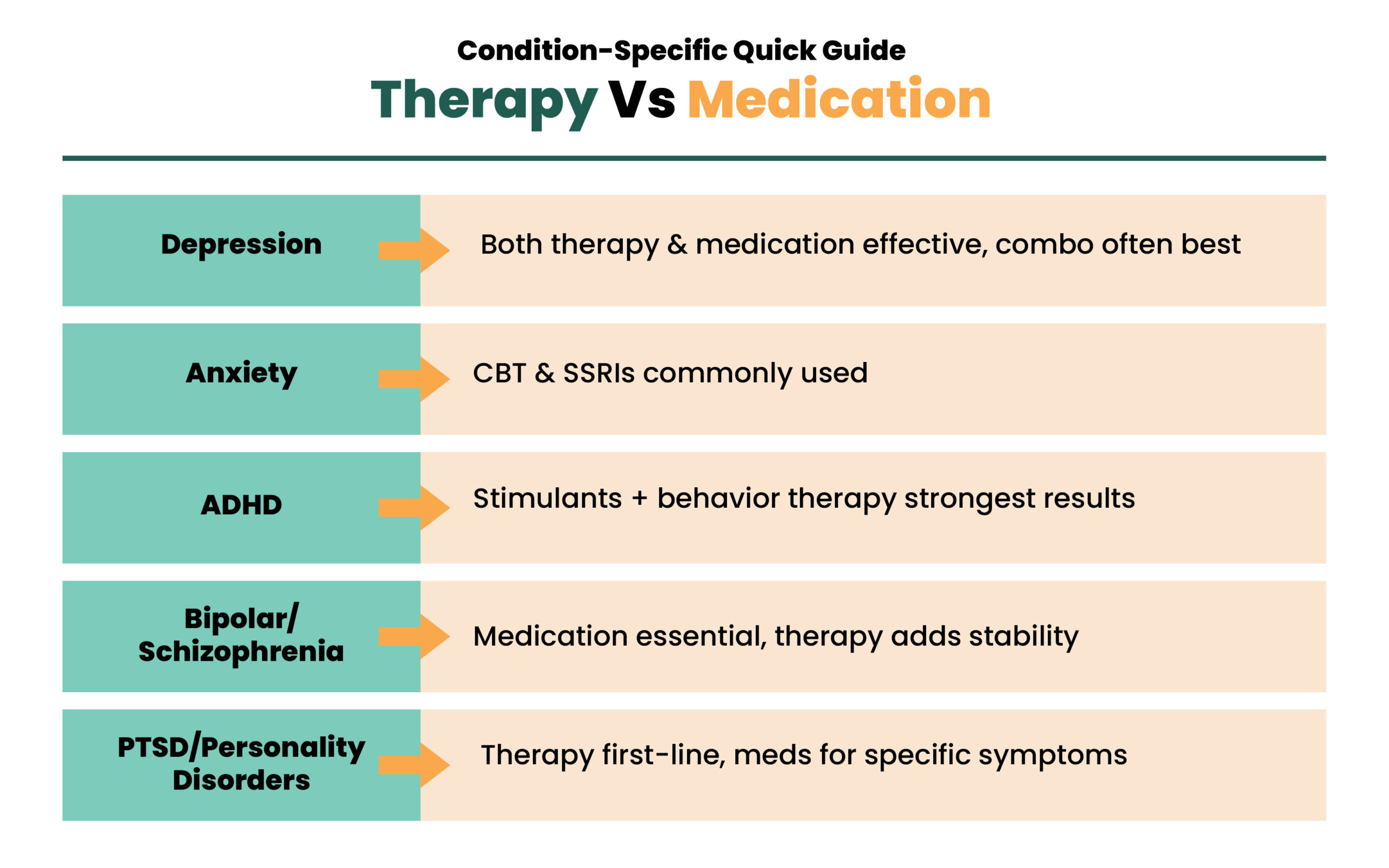
- Anxiety: large meta-analyses show CBT as a top intervention, including for social anxiety and GAD; (ERP) is first-line for OCD, with or without meds.
- Depression: CBT and IPT are effective; for milder episodes, therapy alone is often sufficient.
- PTSD: trauma-focused treatments (e.g., CPT, EMDR, prolonged exposure) are first-line; medicines can help with sleep or mood, but don’t replace targeted trauma work.
- Insomnia: CBT-I is recommended as first-line by major physician groups; sedative-hypnotics are not required for most people.
When Medication Management is Indicated
When symptoms are severe, impairing, or dangerous, online therapy alone hasn’t helped enough, medication is prioritized:
- Bipolar disorder: mood stabilizers form the backbone; therapy is added for relapse prevention and functioning.
- Schizophrenia/psychosis: antipsychotics are essential; therapy aids coping, negative symptoms, and recovery skills.
- Severe or recurrent depression, suicidality, or when agitation, insomnia, or panic attacks block participation in therapy.
- Complex comorbidity where physiology is a significant driver of symptoms.
Medication is not a shortcut; it creates stability so therapeutic work can actually happen.
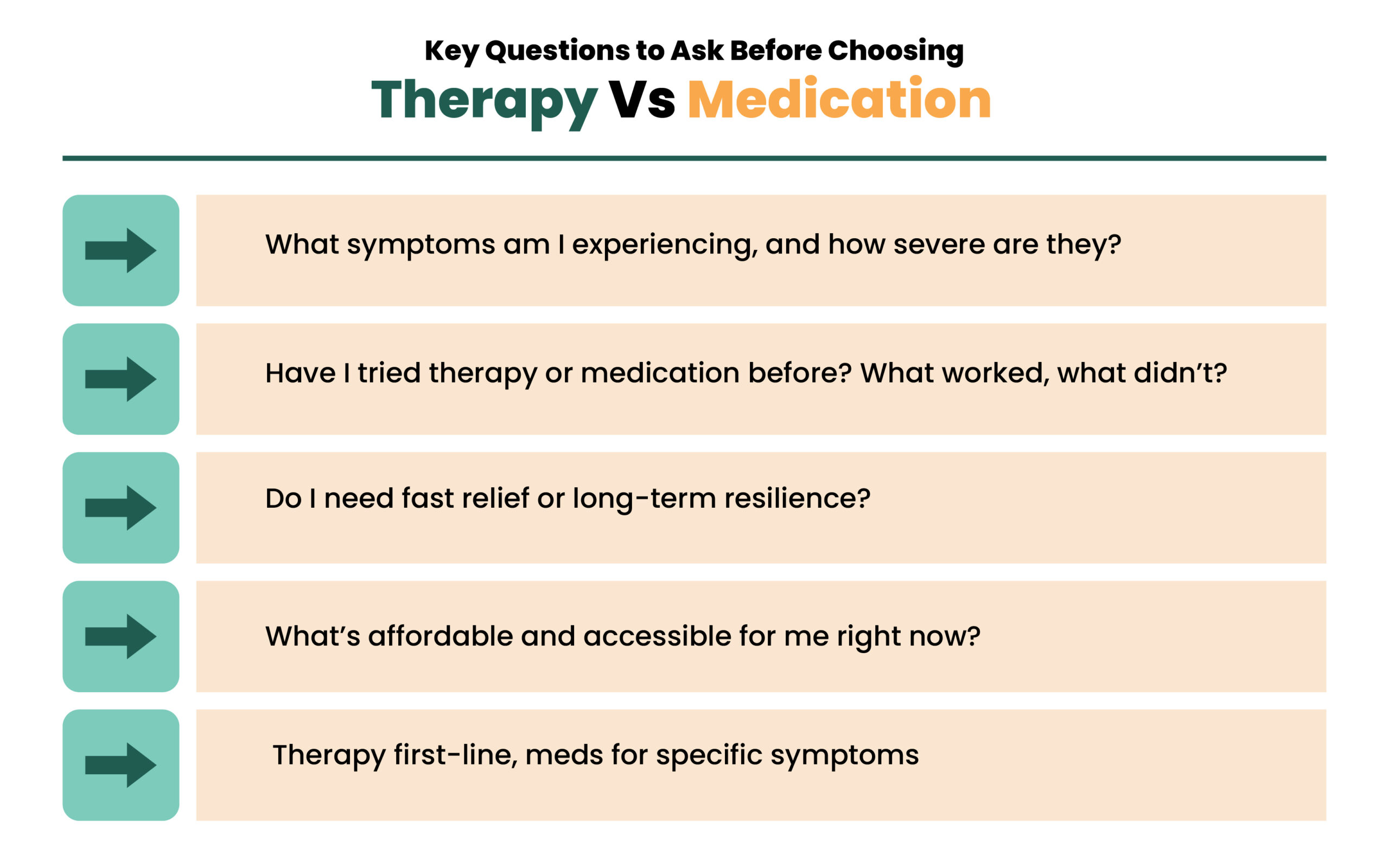
How to Choose: Seven Practical Questions to Decide
Use these to guide a discussion with your clinician:
- Which condition and symptoms are present?
- How severe, how impairing, how urgent?
- Safety needs: do you require fast-acting stabilization?
- What helped or harmed in the past (both therapy and medication)?
- What can you access consistently: qualified clinicians, time, cost, and convenience?
- Do trauma memories, relationship patterns, or habits require talk-through work for resolution?
- Medical factors and drug interactions that influence risk/benefit?
Medication often brings faster symptom reduction; therapy addresses deeper drivers and long-term relapse prevention. Many trajectories use both at different points.
Still Wondering If Therapy or Medication Is Right for You?
You don’t have to guess or struggle alone; the right plan can change everything. Our telehealth/onsite mental health specialists help you decide, simplify your options, and start treatment that actually works for your life.
Symptom Severity and Timing: Fast Relief Vs. Lasting Change
- Crisis or severe symptoms: use medication (and higher-level care if indicated) to stabilize quickly, then transition to (or add) therapy.
- Moderate symptoms: either path is reasonable; combined care if progress stalls.
- Mild or residual symptoms: therapy alone can consolidate recovery and target life goals.
Access, Cost, and Quality: What Actually Sustains Recovery
Cost and logistics decide whether people stay in care. Online medication may be lower cost up-front and easier to maintain through brief medication management visits; therapy may be more cost-effective long-term because skills persist and relapse risk falls. Quality also matters:
- Med response is somewhat more predictable than therapy response, but a good therapist fit can be transformative; a poor fit wastes time.
- Insurance coverage and clinician availability can push choices; the key is staying in effective care, not perfection.
Outpatient Care Across New Jersey & Same-Day Access
CPG operates online & onsite for mental health services (mental health medication management) across New Jersey, with same-day and walk-in appointments. Virtual visits cover evaluation, prescribing, monitoring, and therapy.
Follow-ups are seamless by secure video; in-person services are coordinated locally when a physical exam, labs, or escalated care are needed.
If you’re unsure where to begin, start with a straightforward question set
What are my symptoms, how severe are they, what has helped before, what can I reliably maintain, and what do I need most right now, fast relief, deeper work, or both? Bring those “Questions: to your CPG Televisit; we’ll translate them into a practical plan.
Final Words
Both paths, therapy and medication management, are valid and evidence-based treatments. Therapy helps resolve underlying drivers and builds durable skills. Medication reduces symptom load, protects safety, and enables participation in therapy. Many people do best with both, either at the same time or at different stages.
How we reviewed this article:
CPG experts follow strict sourcing standards, using peer-reviewed research, academic institutions, and trusted medical journals. Only reliable, evidence-based sources are cited to maintain accuracy and integrity.
- https://www.apa.org/practice/resources/evidence
- https://www.nhs.uk/mental-health/talking-therapies-medicine-treatments/talking-therapies-and-counselling/types-of-talking-therapies/
- https://www.apa.org/ptsd-guideline/patients-and-families/cognitive-behavioral
- https://dialecticalbehaviortherapy.com/#:~:text=Overview%20of%20DBT,a%20good%20life%20for%20yourself.
- https://my.clevelandclinic.org/health/treatments/interpersonal-psychotherapy-ipt
- https://www.psychologytoday.com/us/therapy-types/psychodynamic-therapy
- https://www.apa.org/topics/psychotherapy/approaches
- https://iocdf.org/about-ocd/treatment/erp/
- https://pmc.ncbi.nlm.nih.gov/articles/PMC7392659/
- https://my.clevelandclinic.org/health/articles/24946-beers-criteria
Our Review Standards
Our team regularly reviews health and wellness writings. Updates are made on the availability of new & authentic information.
Our Editorial Team
Clinical Adviser:
Author:
