Childbirth is a life-changing experience that is filled with powerful emotions. You have the excitement of having a baby, with fear, worry, and anxiety about how life will be after pregnancy. Within days after childbirth, a mother might experience severe mood swings, extreme sadness, and frequent crying, fatigue, guilt, and loneliness.
These experiences may be postpartum depression, a condition that can affect any woman after childbirth, especially when it’s their first time. Additionally, the expert evaluation of CPG will also rule out the comorbid conditions like
MDD,
PDD, and
Seasonal Affective Disorder, etc.
In this read, we’ll help you understand what postpartum depression is, how it differs from “baby blues,”. Moreover, you’ll also learn about PPD symptoms, causes, and treatment options.
- 1 in 7 mothers experience postpartum depression after birth
- Up to 50% of women never receive a diagnosis or treatment for PPD
- 27.7% of women with postpartum blues developed perinatal depression
What is Postpartum Depression (PPD)?
Postpartum depression (
PPD) is a type of depression that begins within the first year after childbirth. It affects
1 in 7 women and involves extreme sadness, fatigue, guilt, loneliness, frequent crying spells, and severe mood swings.
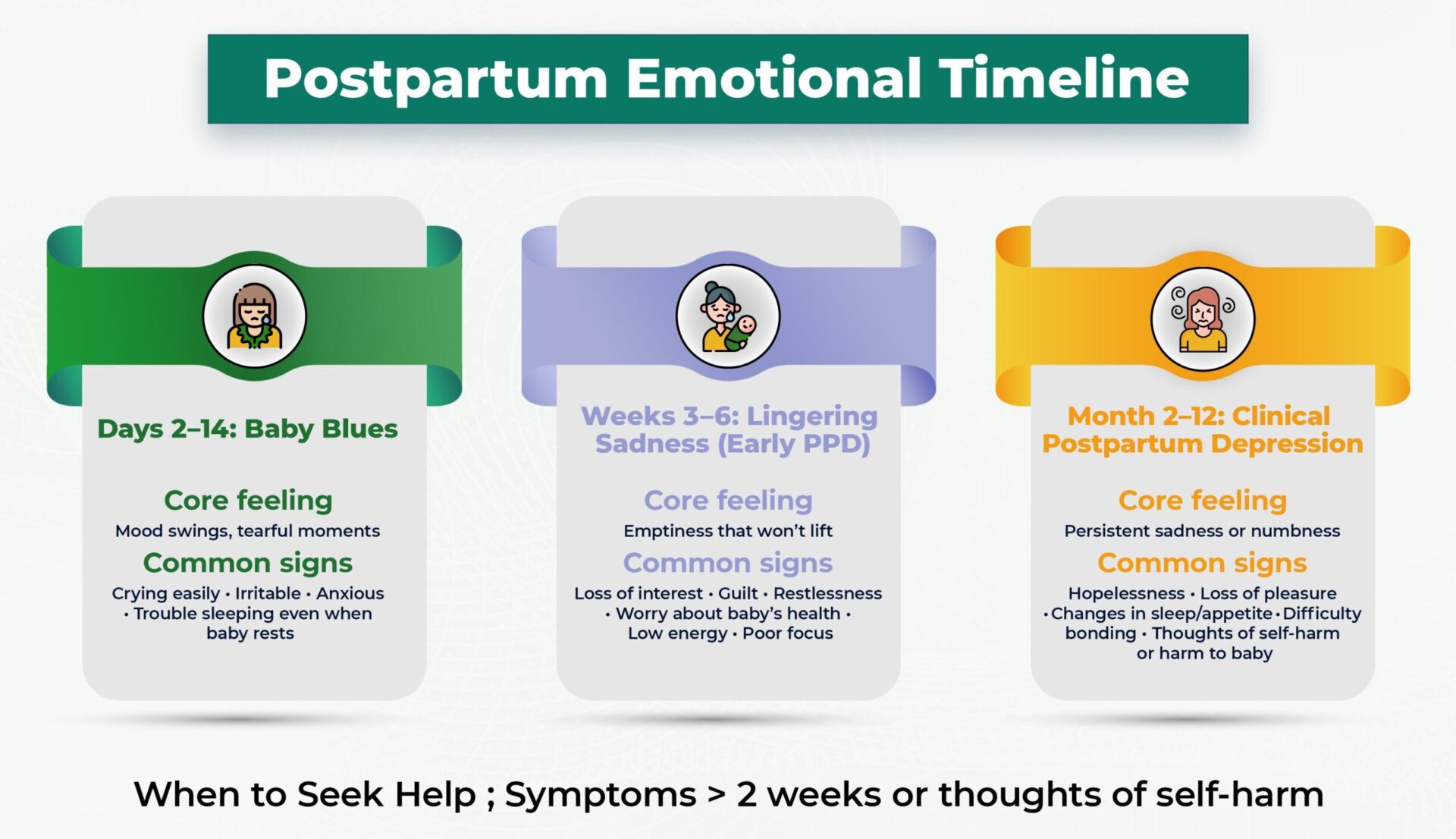
Baby Blues are extremely common and affect up to
70% to 80% of new mothers. It includes mood swings, sleep changes, anxiety, and crying spells, which typically start within the first 2 to 3 days of delivery and last for up to two weeks.
Postpartum depression and baby blue are not weaknesses. It appears because of a hormonal imbalance and other factors, like sleep deprivation and stress that a mother experiences after pregnancy. If you are struggling with any condition, prompt treatment by our mental health professional can help you manage your symptoms.
If sadness, anxiety, or guilt are with you for more than a few weeks, it might be more than “baby blues.” Capital Psychiatry Group’s professionals can clear your doubts and help you bring relief faster than you think.
Baby Blues vs. Postpartum Depression
These two terms, baby blues and postpartum depression, are often used interchangeably, but clinically, they are distinct. In the table below, we’ll show the difference between these two terms.
Postpartum Depression Symptoms (Mild to Severe)
Postpartum depression (PPD) symptoms might make you feel like you are a bad mom, but know that it is extremely common to feel this way after delivery. You don’t have to feel ashamed because you are not the only mother who feels this way after pregnancy.
Below is a breakdown of symptoms/signs of postpartum depression (Mild to Severe):
Mild / Early Signs & Symptoms
These are the milder symptoms that mothers may neglect, thinking it is the stress from taking care of a baby.
- Persistent low or “empty” mood
- Tearfulness for a few days
- Irritability/anger
- Anxiety or intrusive thoughts (about the baby’s health or one’s own)
- Difficulty concentrating
- Fatigue or loss of energy
- Sleep disturbance (insomnia or very fragmented sleep)
- Change in appetite (notably decreased or increased)
When one or two symptoms occur and disappear briefly, then it is normal. But if several signs persist for two weeks or more and start to interfere with self-care and baby care, then you may need to contact a professional for assistance.
Moderate to Severe Symptoms
PPD symptoms might deepen and start to disturb almost all parts of life. These are the severe symptoms that need clinical evaluation and treatment:
- Loss of interest or pleasure (anhedonia)
- Persistent guilt
- Worthlessness
- Excessive self-blame
- Frequent crying
- Difficulty bonding or feeling emotionally connected with the baby
- Thoughts of self-harm or harm to the baby
- Suicidal ideation
- Psychomotor change (noticeable slowing or agitation)
- Marked sleep (very little sleep or hypersomnia)
- Appetite change (very low appetite or overeating)
Recognizing these signs early is the first step toward healing. Our experts at
Capital Psychiatry Group offer personalized assessments and deliver evidence-based care that helps you recover safely and confidently.
What Causes Postpartum Depression?
There is no single cause of PPD. There are many factors contributing to PPD that include:
- Hormonal Changes: During pregnancy, your body has a higher number of hormones. Research has shown that within three days after the pregnancy, hormone levels gradually go back to normal. This change in hormone level might also cause PPD.
- Genes: Studies show that people with a family history of depression are at higher risk.
- Psychological changes: Factors like mental health issues during pregnancy, anxiety before birth, stress in child care, negative emotions, body dissatisfaction, exhaustion, and underweight can also increase the risk of PPD.
How We Diagnose & Screen for PPD
The healthcare provider at CPG may ask questions about your medical/health history, how you have felt since delivery. We might also recommend a physical exam, pelvic exam, and lab tests to have a better understanding of the mother’s postpartum.
Our
mental health professional uses well-recognized and validated screening tools like EPDS and PHQ-9 to measure the severity of symptoms.
Remember that we are here via telehealth & onsite clinics to help and support you in this overwhelming time, so make sure you answer honestly to the questions asked. Your response helps providers differentiate between typical symptoms and postpartum depression symptoms.
Edinburgh Postnatal Depression Scale (EPDS)
The EPDS is a simple 10-question survey about how you’ve felt in the past week after giving birth, focusing mainly on emotional and cognitive symptoms.
Each answer is scored from 0 to 3. The overall score from all questions helps the doctor understand if you are struggling with postpartum depression.
The EPDS is validated in many countries and has been translated into more than 50 languages. The American College of Obstetricians and Gynecologists (
ACOG) recommends its use at postpartum or well-baby visits.
Patient Health Questionnaire-9 (PHQ-9)
The PHQ-9 is a self-filled form that consists of nine questions.
It looks at both emotional and physical changes in women after pregnancy.
Although the PHQ-9 was created for general depression, many experts use the
PHQ-9 as an alternative to EPDS for perinatal and postpartum women.
Just like EPDS, each question has a score. After the test, if your score is 10 or higher, it may suggest that you have moderate to severe depressive symptoms.
Capital Psychiatry Group board-certified professionals use gold-standard screening tools like EPDS and PHQ-9 to identify postpartum depression early. Start a conversation with our professionals to clear your mind.
Postpartum Depression Treatment Options
There are several treatment options for treating PPD, including antidepressant medicine, psychotherapy (CBT and IPT), and support sessions. The
depression treatment plan your provider suggests will be according to the severity of your symptoms.
1. Psychotherapy (Talk Therapy)
Psychotherapy is the first-line treatment option for women with mild-to-moderate peripartum depression. Cognitive Behavioral Therapy (
CBT) and Interpersonal Psychotherapy (IPT) have proven to deliver the most effective treatments for PPD.
Cognitive Behavioral Therapy (CBT)
It helps mothers identify negative thought patterns and replace them with positive thoughts.
Interpersonal Psychotherapy (IPT)
It focuses on managing stress in interpersonal relationships, such as adjustment to motherhood or loss of independence.
2. Antidepressant Medications
Antidepressants are another option to find relief from the symptoms of PPD. They help manage brain chemistry, like serotonin responsible for mood change.
SSRIs as First-Line
To treat moderate-to-severe cases of PPD, Selective Serotonin Reuptake Inhibitors (SSRIs) like sertraline are often prescribed carefully to restore serotonin balance.
Any medication that a breastfeeding mother takes can enter breast milk. Sertraline has a good
safety record, with minimal exposure to infants through breast milk.
Other Antidepressants
Other antidepressants (like SNRIs or atypical antidepressants) may be used if SSRIs are ineffective. They should always be prescribed carefully with proper monitoring.
3. Rapid-Acting Treatments
When needed, other medicines can also be used post-pregnancy for fast treatment. In these cases, two medications are specifically approved by the U.S. FDA for PPD:
Brexanolone
Brexanolone is the first drug approved by the U.S. FDA specifically for PPD. It slows down the rapid drop of certain hormones and reduces depressive symptoms within days. But it can only be used under strict monitoring.
Zuranolone
In August 2023,
zuranolone was approved as an oral neuroactive steroid for PPD. It works similarly to Brexanolone and helps regulate mood.
Note: This is not medical advice and is not equivalent to the doctor’s observations.
In our clinical experience, mothers recover fastest when therapy and medication are combined because they address both the emotions and the brain chemistry.
Why Choose Us for Postpartum Depression Care
Every mother’s experience with postpartum depression (PPD) is unique, and Capital Psychiatry Group understands that the intensity of symptoms and recovery differ for each woman. That’s why we deliver personalized evaluations, diagnosis & treatment via telehealth & in-clinic care that make you feel at home.
- All insurance accepted
- Same-day & weekend appointment
- Walk-in appointments
- Board-certified psychiatrists
- Therapists for postpartum depression
- HIPAA-compliant telepsychiatry
- On-site clinics across NJ
- Evidence-based treatment plans (CBT, IPT & medication)
- Safe medication management during breastfeeding
- Ongoing monitoring and follow-up
Takeaways
Postpartum depression is a medical condition that many women experience after pregnancy. A mother may feel fatigue, guilt, loneliness, worry,
anxiety, crying spells, and extreme mood swings within days after childbirth.
Many mothers feel shame and question their love for the child for feeling these emotions, but remember that PDD and baby blues are extremely common, and you don’t have to feel this way. The problem is rooted in biological, hormonal, psychological, and physical factors that come after childbirth. With awareness, love/support, and proper treatment, PPD is treatable, and recovery is not only possible but common.
Postpartum depression is a treatable medical condition. Our psychiatrists provide compassionate, evidence-based care to help you recover safely.